See also
IgE-mediated food allergy
Anaphylaxis
Eczema
Unsettled or crying babies
Gastro-oesophageal reflux disease in infants
Slow weight gain
Key points
- Non-IgE-mediated food allergies are delayed immune-mediated reactions to food
- Non-IgE-mediated allergies are diagnosed on the basis of clinical history and do not require allergy testing
- Treatment is based on elimination of the trigger food(s), there is no need for adrenaline or antihistamines
- FPIES can lead to dehydration and shock, and may need acute treatment
Background
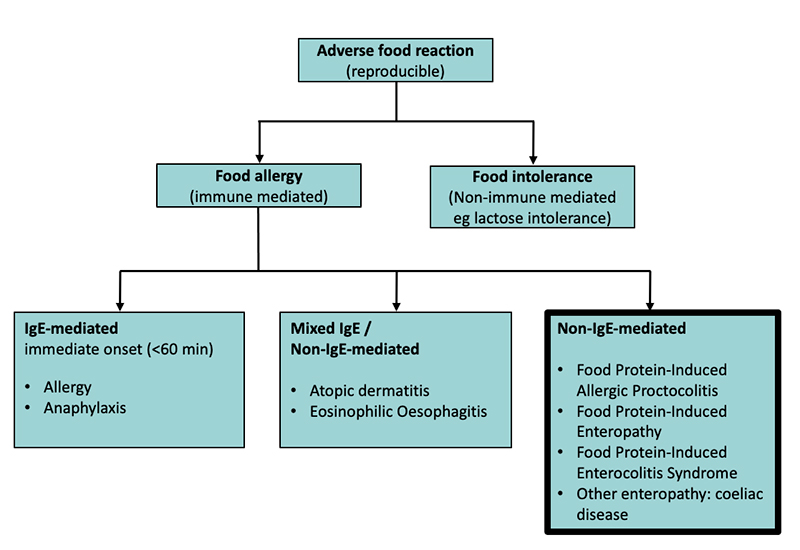
- Food allergies are mediated through the immune system and can be classified as IgE-mediated, non-IgE-mediated, or mixed IgE/non-IgE-mediated
- IgE-mediated reactions are characterized by stereotypical signs and symptoms that develop usually within 60 minutes of ingestion eg urticaria, angioedema, airway compromise (see
IgE-mediated food allergy)
- Non-IgE-mediated food allergies are characterised by a delayed onset of signs and symptoms, usually over hours to days following ingestion
- The exception is FPIES (Food Protein Induced Enterocolitis Syndrome), which occurs on average 2-4 hours after ingestion of the offending allergen
- Non-IgE food allergies are common in the first 1-2 years of life, with most resolving by early childhood
- They commonly involve the gastrointestinal tract
- Non-IgE-mediated allergies do not cause anaphylaxis and therefore are not treated with adrenaline
- CMPI (Cow’s Milk Protein Intolerance) is an umbrella term still used by many clinicians, which encompasses the non-IgE-mediated allergic conditions Food Protein-Induced Allergic Proctocolitis and Food Protein-Induced Enteropathy
Definitions
Food Protein-Induced Allergic Proctocolitis (FPIAP): delayed, non-IgE-mediated inflammation of the rectum, commonly presenting in first few months of life. Stools with blood +/- mucous. Infant usually well and thriving
Food Protein-Induced Enteropathy: delayed, non-IgE-mediated inflammation of the small intestine, commonly presenting in early infancy. Persistent loose stools, vomiting is common and there may be poor weight gain. Child can be unsettled and may have secondary lactose malabsorption, leading to bloating and peri-anal excoriation
Food Protein-Induced Enterocolitis Syndrome (FPIES): delayed onset of repeated vomiting, on average 2-4 hours after ingestion of trigger food. May be associated with pallor, lethargy and may have loose stools. Usually presents in first year of life following introduction of solid foods. The most common trigger foods in Australia are rice, cow milk, soy or oats, however it can be caused by any food. See
ASCIA: Food Protein-Induced Enterocolitis Syndrome (FPIES)
Assessment
History
- Food exposure and timing of reaction (note food may have been ingested directly by the child or through maternal ingestion via breastmilk in FPIAP and enteropathy)
- Has this food been eaten in past, how often, any prior reactions?
- Details of reaction and duration
-
Vomiting
- Diarrhoea
- Stool description, including presence of mucous or blood
- Delayed presentations of lethargy, pallor
- Unsettled behaviour
- Rash (morphology and duration)
- Age at time of initial reaction, timing of other reactions
- Dietary history: breastfeeding (noting any maternal dietary exclusions), formula (including types)
- Growth trajectory, taking note of
slow weight gain
- Associated eczema
- Infectious contacts
Examination
- Assess for dehydration
- Abdominal examination:
- In non-IgE-mediated food allergy presentations, the abdomen should be soft and non-tender
- Consider other causes for presentation if abdomen is distended or tender
- Perianal examination for rash or fissures
- Growth parameters: weight, length, head circumference
- Skin: assess for rashes, ie eczema, petechiae in the setting of bloody stools (consider thrombocytopenia), haemangiomas (may also be present in GI tract and present with rectal bleeding)
Summary of conditions
|
|
Proctocolitis |
Enteropathy |
FPIES |
|
Average age |
<6 months |
<6 months |
<12 months |
|
Vomit |
Usually not prominent |
May be present |
Profuse +++ |
|
Stools |
Blood, mucous usually present |
Mucous +/- blood may be present |
May have loose stools |
|
Lethargy |
No |
Can be present |
Common |
|
Pallor |
No |
Possible |
Common |
|
Hives |
No |
No |
No |
|
Weight gain |
Not affected |
Can be affected |
Rarely affected |
|
Timing of reaction after ingestion |
>few hours-days |
>few hours -days |
Average 2-4 hours |
|
Improvement of symptoms |
Over few days to weeks after eliminating trigger food |
Over few days to weeks after eliminating trigger food |
Once vomiting ceases and fluids tolerated, improvement seen after few hours |
|
Unsettled behaviours |
Usually not present |
May be present |
Not a prominent feature |
|
Common food triggers |
Cow milk, soy |
Cow milk, soy |
Rice, oats, cow milk, soy, eggs |
|
Less common food triggers |
Others not common |
Others not common |
Avocado, chicken, sweet potato, legumes (many others possible) |
|
Differential diagnoses |
- Infectious gastroenteritis
- Early onset inflammatory bowel disease
- Bleeding disorder
|
- Infectious gastroenteritis
- Early onset inflammatory bowel disease
- Coeliac disease (if age > 6 months and child has started solids)
- Underlying immune-deficiency
|
- Infection (sepsis, meningitis, UTI, gastroenteritis) Pyloric stenosis
- Intussusception
- Bowel obstruction (suspect with bilious vomiting)
|
Investigations
- Not routinely required; diagnoses of non-IgE-mediated allergies are made clinically
- If persistent blood in stools, check FBE for anaemia or thrombocytopaenia
- If there are petechiae, suggest urgent FBE looking for thrombocytopenia
- Can consider stool testing for MCS and viral PCR to exclude infectious causes for presentation
- Allergy testing with skin prick tests or allergen-specific IgE testing is not indicated for suspected non-IgE-mediated food allergies
- Allergy testing will not assist with a diagnosis of non-IgE food allergies, and may even cause harm by driving unnecessary food eliminations
- If there is doubt about the diagnosis at the time of an acute presentation and thought to be an allergic cause, discuss with Allergy & Immunology
Management
Proctocolitis and Enterocolitis
Food elimination of suspected trigger
- If cow milk is the suspected trigger, start with cow milk elimination first, noting improvement may not be seen until two weeks
- Includes maternal elimination if child is breast-fed
- If nil or sub-optimal improvement, then also eliminate soy
- It is unusual to need multiple (>2) food eliminations, in which case, a dietitian review is strongly suggested
- Suggest calcium supplements for breastfeeding mother if she is needing to eliminate cow milk and soy
Formula
- If formula is required, suggest trialling an extensively hydrolysed formula (EHF) or rice formula in the first instance
- Recommend two-week trial to begin with
- If no improvements after two weeks of EHF, then change to an amino acid-based formula in consultation with a specialist
- There are a number of over-the-counter formulas available, however some extensively hydrolysed formulas and all amino acid-based formulas require a prescription
- If no improvements on amino acid-based formula, re-evaluate for alternative diagnosis
- Ongoing monitoring of weight gain is important
Re-introduction of foods
- Consider re-introduction of trigger foods, one at a time, around 12 months of age
- Recommend at least 2-3 week interval between each food introduction
- For cow milk re-introduction, suggest a graded approach starting with processed milk (eg milk in baked goods), then hard cheese, yoghurt and then finally fresh milk
- If any delayed reactions occur, cease introduction and re-try in another few months
- Most children will improve by 1-2 years of age
FPIES
Acute management:
- Treat
vomiting
- Suggested ondansetron doses (oral):
|
Weight |
Dose |
|
8-15 kg |
2 mg |
|
15-30 kg |
4 mg |
|
>30 kg |
6-8 mg |
- Fluid resuscitation (see
Intravenous fluids)
- In an unwell child, or if not improving with initial management, have a low threshold to investigate and treat for other possible causes, such as
sepsis
- Any bilious vomiting requires an urgent surgical opinion
Long term management
- Prior to discharge, the family should be given an
FPIES Action Plan and a script for ondansetron
- Food elimination of suspected trigger
- Suggest referral to a paediatric allergist
- Most cases resolve by 2-3 years of age
- A paediatric allergist usually manages re-introduction of trigger foods, as some of these need to be done under medical supervision
Consider consultation with local paediatric team when
- If no improvements in symptoms with common food eliminations, then refer to general paediatrician, paediatric gastroenterologist or paediatric allergist/immunologist
- If poor weight gain, loose stools and eczema, and not responding to treatment, consider referral to Immunology to exclude other causes (an underlying primary immune-deficiency, eg SCID, may present in this way)
Consider transfer when
Any child requiring care beyond the level of comfort of the treating hospital
For emergency advice and paediatric or neonatal ICU transfers, see
Retrieval Services
Consider discharge when
Parental education has occurred and written/printed advice provided. See Parent Information (below)
Appropriate follow-up has been arranged
For FPIES: when the child is tolerating oral fluids and appears well
Parent information
ASCIA: Food Protein-Induced Enterocolitis Syndrome (FPIES)
ASCIA: Food Protein-Induced Allergic Proctocolitis (FPIAP)
Additional resources
ASCIA: FPIES Action Plan
ASCIA: Guide for Milk Substitutes in Cow’s Milk Allergy
Last updated October 2022